
From the 1Department of Health Sciences, Lund University, 2Department of Rehabilitation Medicine, Skåne University Hospital, Lund, 3Department of Neurobiology, Care Sciences and Society, Division for Clinical Geriatrics, Karolinska Institutet Stockholm and Aleris Rehab Station R&D unit, Solna, 4Region Norrbotten, Sunderby Research Unit, Development department, Luleå, 5Spinalis Foundation, Stockholm, 6Department of Rehabilitation Medicine, Linköping University Hospital, 7Department of Health, Medicine and Caring Sciences, Linköping University, Linköping, Sweden
Objective: To describe data completeness, targeting and reliability of the Swedish version of the Spinal Cord Independence Measure Self-Report (s-SCIM-SR).
Design: Translation and reliability study.
Subjects: Programme participants (n = 48) and peer mentors (n = 42) with spinal cord injury enrolled in the INTERnational Project for the Evaluation of “activE Rehabilitation” (inter-PEER).
Methods: The translation process was based on guidelines/recommendations, and involved expert competence, including consumers. The s-SCIM-SR was distributed online, once for programme participants and twice for peer mentors.
Results: Sixty-nine individuals (77%) obtained a total score. Most missing data were found in the items Respiration and Using the toilet. Cronbach’s alpha for the full scale was 0.89, for Self-care 0.92, for Respiration and sphincter management 0.37 and for Mobility 0.86. The intraclass correlation coefficient was excellent for all subscales and the full scale. Measures of variability showed high sensitivity to changes and Bland Altman analyses revealed no systematic changes between evaluation points.
Conclusion: These results support the data completeness, targeting and reliability of the Swedish version of the SCIM-SR. However, some problems were found in the subscale Respiration and sphincter management. The s-SCIM-SR can be considered psychometrically sound and suitable to assess physical independence among persons with spinal cord injury in Swedish community settings.
Key words: outcome measures; psychometrics, rehabilitation; spinal cord injury.
Accepted Apr 20, 2021; Epub ahead of print May 5, 2021
J Rehabil Med 2021; 53: jrm00197
Correspondence address: Sophie Jörgensen, Department of Health Sciences, Rehabilitation Medicine Research Group, PO Box 157, Lund University SE-221 00 Lund, Sweden. E-mail: sophie.jorgensen@med.lu.se
Doi: 10.2340/16501977-2839
After spinal cord injury, an important goal in rehabilitation is to attain a high level of physical independence. In Sweden, no spinal cord injury-specific assessment tool to evaluate physical independence has previously been nationally available. This study presents the translation process and evaluation of the measurement properties of the Swedish version of the Spinal Cord Independence Measure Self-Report (s-SCIM-SR) in a community rehabilitation setting. The translation process involved expert competence, including consumers, and resulted in minor cultural adaptations. The s-SCIM-SR was distributed online to 90 persons with chronic spinal cord injury. Overall, the s-SCIM-SR performed equally as well as the original version in terms of missing data, general agreement between items, and agreement between 2 evaluation points. However, some problems were found in the subscale Respiration and sphincter management. In conclusion, the s-SCIM-SR can be considered psychometrically sound and suitable to assess physical independence among persons with spinal cord injury in Swedish community settings.
Sustaining a spinal cord injury (SCI) can be a life-altering event, and often results in a variety of impairments, activity limitations and participation restrictions. A major goal in rehabilitation after SCI is to attain a high level of physical independence. In order to assess the effectiveness of interventions and to monitor spontaneous improvements, valid and reliable measures are needed (1) to evaluate functioning and disability over time after SCI, in both inpatient and community rehabilitation settings.
The Spinal Cord Independence Measure (SCIM) (2) is a SCI-specific measurement of independence in daily activities, taking into account the time needed to perform the activities, the difficulty and the subjective value of tasks performed (3). The current third version comprises 19 items covering 3 domains of activities of daily living: self-care, respiration and sphincter management, and mobility (4); and has shown satisfying psychometric properties (4–6). The SCIM has been suggested to be the primary outcome measure of functional recovery after SCI (7). It was originally developed by Catz and co-workers as a clinician-administered assessment based on observation (2), and is therefore time-consuming and resource intensive. For research purposes, the tool is often used as an interview, resulting in slightly decreased precision due to variability between raters (8) and a general risk of the respondent to over- or under-rate their performance.
To overcome these barriers and facilitate data collection in community settings, a self-report version was developed by Fekete et al. (9), the SCIM Self-Report (SCIM-SR). Fekete et al. adapted the wording in SCIM III by using personal pronouns and avoiding or explaining technical terms. Several complex items were divided into simpler components and a scoring algorithm was developed to obtain consistency with SCIM III. Another separate and less widely-received attempt to develop a version of SCIM III for self-report use was performed by Michailidou et al. (10). This version included only simple grammatical adjustments without making adaptations that would facilitate self-reporting (11). In Europe, the German (9), Spanish (12), and Italian (13) translations of the SCIM-SR have shown satisfying criterion validity compared with the clinician-administered versions. Neither SCIM-SR nor SCIM III have previously been nationally available in Swedish. Moreover, European versions of the SCIM-SR have neither been evaluated for test-rest reliability nor tested in a community rehabilitation setting.
We recently initiated the INTERnational Project for the Evaluation of “activE Rehabilitation” (Inter-PEER) (14), a collaboration between an international team of researchers and the non-profit organizations using the Active Rehabilitation (AR) concept. AR is a community rehabilitation concept, based on the use of peer mentors as trainers and educators. Inter-PEER is a prospective cohort study with the primary aim to assess the effects of AR training programmes on community-dwelling individuals with SCI with regard to physical independence, wheelchair skills, participation, life satisfaction, level of physical activity, resilience, and self-efficacy (14). As part of Inter-PEER, we translated and culturally adapted the SCIM-SR into Swedish (s-SCIM-SR). The aim of the present study is to describe the psychometric properties regarding data completeness, targeting and reliability of the s-SCIM-SR in a community setting.
Spinal Cord Independence Measure Self-Report
Similar to the SCIM III, the SCIM-SR consists of 3 subscales: the Self-care subscale comprises items 1–4 (0–20 points), the Respiration and sphincter management subscale comprises items 5–8 (0–40 points), and the Mobility subscale comprises items 9–17 (0–40 points). The possible total score is 0–100, where 0 represents total assistance in all activities and 100 represents maximal independence with no need for assistance or adaptive devices. The items are graded and weighted to capture the difficulty of performance, the subjective value of the activities and the time required (3). The Rick Hansen Institute developed a toolkit to improve scoring clarity and inter-rater reliability of the SCIM III (15). The SCIM III has shown good test-retest reliability and a Cronbach’s alpha of >0.70 for all subscales and 0.85 for the total scale (4). It is used both in research and clinical practice, and is sensitive to detect changes during primary rehabilitation (16). The SCIM-SR was developed by investigators familiar with the SCIM III and was scrutinized by external experts, such as the developer of the SCIM III and persons with SCI (9). Further details about the process can be found in Fekete et al. (9).
Participants and data collection
The Inter-PEER commenced in Sweden in 2018 and includes participants in AR training programmes that last for a minimum of 7 days. The research project is designed to be fully integrated into the AR programmes (for details, see Divanoglou et al. (14)). All participants in the Swedish AR training programmes are invited to participate in the Inter-PEER, providing they meet the following inclusion criteria: (i) having a SCI (traumatic, non-traumatic, or congenital, e.g. spina bifida); (ii) being 16 years or older; (iii) being able to comprehend and answer written questions in Swedish and (iv) being able to independently push a manual wheelchair for at least 25 m on an even surface (applicable for wheelchair users) (14).
Participants in Inter-PEER are invited to complete a battery of 10 standardized assessments (including, for example, the s-SCIM-SR and self-reported sociodemographic and injury characteristics) through an online survey, and wheelchair users are invited to perform a practical wheelchair skills test. The online survey was carried out at 3 specific evaluation points: on the first day of the programme (baseline), at the end of the programme, and 3 months afterwards. At the first and second evaluation points, a research assistant was available to clarify any issues when completing the online survey. Based on feedback during the pilot implementation of the Inter-PEER survey, and with the aim of reducing the complexity and time for survey completion, we chose to keep the format of the online questionnaire as simple as possible (14). Therefore, we removed any logic rules, such as making it mandatory to answer specific questions, and applying jump-rules for items in bladder, bowel and mobility. The current study includes secondary analysis of the baseline data for all Swedish-speaking participants with SCI in Swedish AR programmes during 2018.
To enable a more thorough assessment of the s-SCIM-SR, all Swedish-speaking peer mentors with SCI who participated in AR training programmes during the period 2013–18 were invited to complete the baseline survey. To assess test-retest reliability, peer mentors were invited to complete the online survey twice, with a 1 or 2-week interval (T1 and T2). The peer mentors were all considered to have a stable level of function.
Ethics
The participants received both written and oral information about the study before enrolment, and provided written informed consent to participate. The study protocol has been approved by the Swedish Ethical Review Authority (approval number 2018/313-31/5; 2019-01032), and the principles of the Declaration of Helsinki for research on humans were followed throughout the course of the research.
Translation process
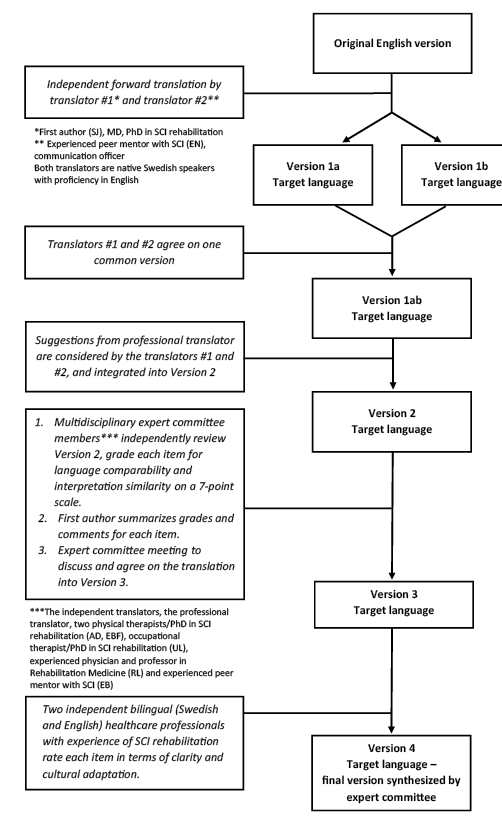
The overall translation process for translating outcomes measures used in the Inter-PEER is described in Divanoglou et al. (14). Fig. 1 describes the specific process for the s-SCIM-SR. The developers of the SCIM-SR (9) were contacted, and provided permission for translation into Swedish. To ensure a high level of accuracy in linguistic translation and cultural adaptation, a process based on previously published guidelines and recommendations was used (12, 17–20), inspired by Fekete et al. (21) and Wahman et al. (22).
Fig. 1. Translation process of the Swedish version of the Spinal Cord Independence Measure Self-Report (s-SCIM-SR)
Statistical analyses
Data completeness. It is important to determine the extent of missing data, as a sum score cannot be confidently estimated if there is a large amount of missing data (23). In addition, if 1 item exhibits many missing values, there might be a problem with either the original item or the translated version (23). Data completeness for the s-SCIM-SR was evaluated by calculating the percentage of missing data for each item, for each subscale and for the total score at the first evaluation point.
Targeting. For the s-SCIM-SR, targeting was evaluated by examining score distributions, together with floor and ceiling effects. Floor and ceiling effects refer to the percentage of participants scoring the lowest and the highest possible score, respectively, and should not exceed 15% (23).
Reliability. Reliability refers to the extent to which a scale gives accurate and consistent results that are not a result of random error (23). Internal consistency reliability of the s-SCIM-SR was evaluated using the Cronbach’s alpha coefficient, for each subscale and for the full scale. Cronbach’s alpha should exceed 0.70 for the scale to be considered internally consistent (23).
Test-retest reliability for the s-SCIM-SR was evaluated using 3 types of analyses: the intraclass correlation coefficient (ICC), the percentage of agreement between the 2 evaluation points and the weighted kappa (23). ICC is a measure of the ratio of variability between individuals to the total variability (i.e. the variability between individuals and the measurement error). ICC was used to determine the agreement of the total score and the scores for each subscale between evaluation points. An ICC ≥ 0.75 represents excellent agreement. Unlike percentage agreement, the weighted kappa coefficient determines the proportion of agreement beyond that expected by chance. A weighted kappa of 0 thus represents that the agreement is no better than chance, and a value of > 0.75 represents excellent agreement. Weighted kappa for each individual item was computed by assigning quadratic weights. To evaluate whether there was a systematic error in scoring, we reviewed and compared the mean and median scores of all items where the weighted kappa was less than 0.60 (representing moderate agreement) and complete agreement less than 90%.
To assess the variability of the subscales and the full scale, the standard error of measurement (SEM) was calculated using the formula standard deviation (SD) (baseline) × √1–reliability (24). The SEM represents the limit for detecting a real change in a group of individuals. From the SEM, the smallest detectable difference (SDD), representing a real change for a single individual, was calculated using the formula SEM × 1.96 × √2 (25).
To assess systematic changes of the mean in all subscales and the full scale between the evaluations points, Bland-Altman analyses (26) were performed including the mean difference (d), the 95% confidence interval (95% CI) around d and the limits of agreement (LOA). For no systematic difference between test occasions, the CI should include 0 (27). The LOA (ranging between d–1.96 × the standard deviation of the differences (s) and d + 1.96s) represents the interval within which 95% of the differences of the mean lie and can be used to illustrate the clinical importance of the differences (26).
Sociodemographics and injury characteristics
A total of 90 persons were included in the study, of whom 48 were programme participants and 42 peer mentors. All 48 Swedish speaking programme participants (30 men, 63%) in the Swedish AR training programmes that took place during 2018 consented to Inter-PEER and were included in the current analysis (response rate 100%) (Table I). Their median age (IQR) was 44.5 years (30), and median time since injury (IQR) 1 year (2). Of the 48 participants, 48% (n = 23) presented with paraplegia, 35% (n = 17) had a complete injury and 77% (n = 37) had sustained a traumatic injury.
Out of 45 peer mentors meeting the inclusion criteria, 42 completed the survey (31 men, 74%) and were included (response rate 93%). Their median age (IQR) was 38.5 years (18) and their median time since injury (IQR) was 10 years (9). In total, 76% (n = 32) presented with paraplegia, 50% (n = 21) had a complete injury and 88% (n = 37) had sustained a traumatic injury.
Table I. Sociodemographic and injury characteristics of participants in Active Rehabilitation programmes and active peer mentors
Swedish version of the Spinal Cord Independence Measure Self-Report
Translation process. The final translated version is shown in Appendix S1. Overall, there were no major disagreements between members of the expert committee. Items were in general easy to adapt to Swedish conditions. The major issues encountered during the process were: (i) the English term “assistance” can, in Swedish, refer to personal assistance provided by employed staff. Therefore, the committee agreed on using the more general Swedish term for “help” to avoid any misinterpretation; (ii) in the Mobility subscale, the expert committee agreed on adding the word “rollator” (i.e. 4-wheeled walker) to the Swedish version as this walking aid is very common in Sweden; (iii) for item 9 (“How many of the following activities can you perform without assistance or electrical aids?”), the English version contains the activity “doing push-ups in wheelchair” which cannot be translated verbatim into Swedish. The expert committee therefore agreed on adding the clarification “for pressure relief” according to clinical practice in Sweden; (iv) for item 15 (“Going up and down stairs”), the expert committee discussed whether the scoring referred to managing stairs in general (e.g. using a wheelchair) or to managing stairs on foot. After consulting the Toolkit for SCIM III (15), which confirmed that the scoring refers to managing stairs on foot, it was decided to use the Swedish term for walking instead of the Swedish equivalent to “going up and down stairs” to ensure comprehensibility. The 2 independent bilingual healthcare professionals perceived the level of clarity as equivalent to the English version. Furthermore, the cultural adaptation was perceived as very good and no major remarks were made.
Scoring. The mean (SD) [min–max] total score for programme participants was 61 (SD 19) [21–100], for peer mentors 68 (SD 15) [24–95] and for the total group 64 (18) [21–100] (Table II).
Table II. Scores on the Swedish version of the Spinal Cord Independence Measure Self-Report (s-SCIM-SR) in participants in Active Rehabilitation programmes and peer mentors
Data completeness. Forty-two out of 48 (88%) participants of the AR training programmes had answered all items in the s-SCIM-SR and obtained a total score (Table III). In total, 6 participants had left 1 item blank (5 participants for item 5 (“I do not need a respiratory (tracheal) tube…”); response rate 90%, and 1 participant for item 7(a) (“Bowel management; Do you need assistance with bowel management?”); response rate 98%. The response rates for all other items were 100%. Missing data were hence found in the subscale Respiration and sphincter management with a response rate of 88%.
Twenty-seven out of 42 (64%) peer mentors answered all items in the s-SCIM-SR at T1 (Table III). Most missing data were found in item 5 (“I do not need a respiratory (tracheal) tube…”) with a response rate of 83%, and item 8 (“Using the toilet”) with a response rate of 76%. Missing data were hence found in the subscales Respiration and sphincter management and Mobility, with response rates of 67% and 93%, respectively.
Table III. Valid and missing responses for all items in the Swedish version of the Spinal Cord Independence Measure Self-Report for participants in Active Rehabilitation programmes (baseline) and peer mentors (Τ1*)
Targeting. With regard to the programme participants, the subscales and the full scale spanned a large range of possible scores; the Self-care subscale ranged from 2 to 20 (full range 0–20), the Respiration and sphincter management subscale ranged from 13 to 40 (full range 0–40), the Mobility subscale ranged from 5 to 40 (full range 0–40) and the full scale ranged from 21 to 100 (full range 0–100). No programme participant scored the lowest possible score on any subscale. Ceiling effects were noted in the Self-care subscale where 19% of the programme participants scored the highest possible score. For the other subscales and the full scale, 2% of the programme participants scored the highest possible score.
With regard to the peer mentors, the Self-care subscale ranged from 2 to 20, the Respiration and sphincter management subscale ranged from 16 to 39, the Mobility subscale ranged from 3 to 40 and the full scale ranged from 24 to 95. No peer mentor scored the lowest possible score on any subscale. Ceiling effects were noted in the Self-care subscale where 52% of the peer mentors scored the highest possible score. For the Mobility subscale, 5% scored the highest possible score.
Reliability
Internal consistency. With regard to the programme participants, the Cronbach’s alpha coefficient for the full scale was 0.88, for the Self-care subscale 0.91, for the Respiration and sphincter management subscale 0.40 (where the alpha-value increased to 0.48 when item 5 (“Respiration”) was deleted) and for the Mobility subscale 0.89 (Table IV).
With regard to the peer mentors, the Cronbach’s alpha coefficient for the full scale was 0.84, for the Self-care subscale 0.92, for the Respiration and sphincter management subscale 0.27 (where the alpha-value increased to 0.50 when item 7 (“Bowel management”) was deleted) and for the Mobility subscale 0.81.
Table IV. Internal consistency reliability of the Swedish version of the Spinal Cord Independence Measure Self-Report for participants in Active Rehabilitation programmes and peer mentors, as measured by the Cronbach’s alpha coefficient
Test-retest reliability
Test-retest (Table V) was performed for peer mentors exclusively, and the ICC for the full scale was 0.98 (n = 18), for the Self-care subscale 0.89 (n = 36), for the Respiration and sphincter management subscale 0.90 (n = 20) and for the Mobility subscale 0.96 (n = 33). The lowest value for the weighted kappa was found in item 5 (“Breathing”): 0.47, and the highest in item 6b (“Bladder management, Intermittent catheterization”): 1.00. In total, 11 items had a weighted kappa value of ≥ 0.75. When comparing the mean and median score for each item for test and retest, none of the items reached statistical significance, indicating no systematic error in the ratings.
Table V. Test-retest reliability of the Swedish version of the Spinal Cord Independence Measure Self-Report for peer mentors in Active Rehabilitation programmes, as measured by weighted kappa and % of complete agreement
Variability and systematic changes of the mean
The SEM and SDD for the full scale were 1.9 and 5.3, respectively (for all subscales, see Table VI). The ds for the full scale and all subscales were close to 0 and the 95% confidence interval included 0, indicating no systematic differences between the evaluation points. The LOA ranged between –7.55 and 6.43 for the total scale (for all subscales, see Table VI). In Fig. 2, the Bland Altman plot of the individual differences in the total score between the 2 evaluation points are plotted against the mean of the 2 evaluation points.
Table VI. Standard error of measurement (SEM), the smallest detectable difference (SDD), the mean difference between test occasions (d), 95% confidence interval (95% CI) of d and limits of agreement (LOA) for the Swedish version of the Spinal Cord Independence Measure Self-report for peer mentors in Active Rehabilitation programmes
Fig. 2. Bland–Altman graph showing individual differences in the total score of the Swedish version of the Spinal Cord Independence Measure Self-Report (s-SCIM-SR) between evaluation points plotted against the individuals’ mean of the two evaluation points.
This study describes the translation and adaptation process of the Swedish version of the SCIM-SR and explores its psychometric properties (data completeness, targeting and reliability) in a community setting. The translation process resulted in minor cultural adaptations to avoid misinterpretations. Generally, the s-SCIM-SR exhibited as good psychometric properties as the original version with high internal consistency, high test-retest reliability, high sensitivity to changes and no systematic changes between evaluation points. However, some problems were found in the subscale Respiration and sphincter management. The study included 90 persons with SCI: 48 participants and 42 peer mentors in AR rehabilitation programmes and nearly 8 out of 10 (77%) answered all items.
Study participants and translation process
The sample size of 48 programme participants and 42 peer mentors was in line with previous research (9, 12, 13, 28) (n = 86–116), they had a broad range of age (17–74 years), time since injury (0–44 years) and severity of SCI, and presented with different levels of independence. This provided a solid ground for the testing process. The thorough translation process was performed according to guidelines (17–19). As the consumer perspective is a central part in developing and evaluating self-reported outcome measures, the translation process, and the manuscript preparation, comprised persons with SCI.
In self-reported outcome measures, items must be clear and easy to understand. As there is a lack of formal instructions for the SCIM III and SCIM-SR, and as the wording of the outcome measure is rather minimalistic, there is a risk of possible misunderstandings. During the translation process, 2 items related to different walking aids and stair management resulted in discussions. To avoid misinterpretation, the walking aid “rollator” (4-wheeled walker) was added to the Mobility section, and the scoring instructions regarding stair management were slightly modified to clarify that the item clearly refers to stair management on foot and not in a wheelchair (as highly skilled wheelchair users might manage some stairs). The toolkit developed by Rick Hansen Foundation, and approved by the developer of SCIM-III, is useful for also clarifying issues regarding the self-report version. However, as it is not directly connected with the outcome measure itself, it may not be easily located by clinical professionals or researchers. Refining instructions for SCIM has been suggested earlier by Ackerman et al. (16) and training of clinicians has been requested (29).
Data completeness and targeting
There were almost no missing data, except in the subscales regarding respiration and bowel and bladder management. Most missing data were found in items assessing respiration, where peer mentors reported missing data to the highest extent (17%, programme participants 10%). As three-quarters of peer mentors had a paraplegia there is a possibility that they did not experience any problems related to respiration and therefore may not have regarded the item as relevant. Furthermore, there might be general embarrassment to state problems regarding bowel and bladder issues, something that also has been recognized by Fekete et al. (9), who found most missing data in the bladder item (5%), followed by the dressing items (2%). Bonavita et al. (13) reported no missing data, and Aguilar Rodrigues et al. (12) did not report information about missing data. As the present study involved data collection using an online survey in community settings (training programme for programme participants and at home for peer mentors), whereas the other studies were conducted within clinical settings, the willingness to answer the questions might differ.
The item “Using the toilet” exhibited a particularly large difference in missing data between programme participants and peer mentors (0% and 24%, respectively). When scrutinizing the scoring options, it might be somewhat difficult to differentiate between the options “I do not need assistance but I need adaptive devices (e.g. bars) or a special setting (e.g. wheelchair accessible toilet)” (4 points) and “I do not need any assistance, adaptive devices or a special setting” (5 points). A person might be independent in their own home without any adaptive devices or special setting, but in public areas he/she might need a wheelchair accessible toilet, as public toilets are generally not spacious enough to enter in a wheelchair. It is likely that peer mentors would have encountered problems with inaccessible public toilets to a greater extent than programme participants.
In general, peer mentors had more missing data than did programme participants. The engagement in answering the survey might be lower for persons who do not have any previous experience with the survey and who complete it on their own at home, compared with those who receive guidance. Moreover, programme participants had the possibility to ask questions if items were perceived as unclear, which might also have had an impact on the response rate. It is uncertain if this reflects a problem with online self-reported surveys in general or the s-SCIM-SR in particular.
In the total score, there were neither floor nor ceiling effects, but ceiling effects were noted in the Self-care subscale for both programme participants and peer mentors. This could possibly be explained by selection bias as persons with need of total assistance or those completely independent do not choose to join this kind of community rehabilitation programmes. Another possible explanation for ceiling effects in the Self-care subscale, is that persons with SCI in Sweden have access to comprehensive rehabilitation within public health care, and, in general, achieve a high level of self-care early after the injury. As a comparison, Ackerman et al. (16) did not report ceiling effects in the total scores, but in specific items in Respiration for all but persons with C1–C4 injuries, in Feeding and grooming for persons with C7–T12 injuries, and in Dressing upper body and some aspects of Mobility for persons with paraplegia. They included exclusively persons with motor complete injuries (American Spinal Injury Association Impairment Scale (AIS) A and B), compared with the current study, which included a more diverse group in terms of lesion completeness. Ceiling effects were also revealed in the Mobility subscale for peer mentors. This was expected, as peer mentors are required to be well-skilled. Therefore, we do not consider these latter ceiling effects as problematic for the outcome measure.
Reliability
Regarding internal consistency, the same pattern was revealed for both programme participants and peer mentors with lower Cronbach alpha values for Respiration and sphincter management (0.27 and 0.40, respectively compared with the other subscales with Cronbach’s alpha ≥ 0.81). This is in line with previous studies (28, 30, 31), suggesting that these items correlate poorly with each other. The findings are not surprising, as items assessing independence in very different domains (respiration vs bladder and bowel management) are grouped together. In addition, the items assessing bowel management include questions about bowel movements and faecal incontinence, which are related to bowel functioning and not to independence.
Supporting the test-retest reliability, an ICC well over 0.75 (0.89–0.96) was shown for the 3 subscales (Self-care, Respiration and sphincter management, and Mobility). These results are in line with previous results (Glass et al. (28) > 0.84). However, the weighted kappa was ≥ 0.75 in only 11 out of 19 items. For items Eating and drinking (1a), Breathing (5), and Bowel management (7a), the weighted kappa was considered poor <0.5. Post-hoc analysis showed no signs of a systematic error. Overall, the translated scale seems to work well at a sub-scale and total sum level.
The SEM for the full scale was close to 2 points and between 0.5 and 1.8 points for the subscales. Moreover, the SDDs ranged from 1.5 to 5.3. These results indicate that the s-SCIM-SR should be sensitive enough to detect a change in physical independence; for example, following an intervention or over time, both within a group and for a single individual.
As shown in Table VI and Fig. 2, the mean differences between the 2 evaluation points in the subscales and the full scale were small. In addition, 95% of the differences (represented by the LOA) lay within 14 points. Considering the large range of possible scores (i.e. 0–100), the differences between evaluation points can be considered small.
Study limitations
This study has some limitations. First, as the study was performed in a community setting at the AR training programme, inevitably participants may be more motivated when it comes to rehabilitation than the general SCI population. Also, due to the inclusion criteria of the AR programmes and the Inter-PEER, persons with the most severe SCI (i.e. those using ventilators or full-time users of power wheelchair) were not included in this study. Nevertheless, participants did cover a broad range of SCIM scores, including rather low (minimum–maximum 21–100/100).
Secondly, the SCI characteristics of the participants were self-reported. However, all reported data regarding level and completeness of SCI were screened by a physiotherapist and found plausible. Self-reported SCI data have earlier been used in large surveys and shown to be consistent with medical records (32).
Thirdly, there were some missing data in the items Respiration, and Bladder and bowel management, mostly for peer mentors. Missing items can be due to for example challenging items either in the original version or the translated version. Nevertheless, we consider the extent of missing data low enough to verify the reliability of the Swedish version of the SCIM-SR.
Conclusion
The results of this study support the data completeness, targeting and reliability of the Swedish version of the SCIM-SR. However, some problems were found in the subscale Respiration and sphincter management. The tool was translated through a rigorous, consumer-involved process to ensure a high accuracy in linguistic translation and cultural adaptation. The s-SCIM-SR can be considered a psychometrically sound and suitable outcome measure to assess physical independence among persons with SCI in Swedish community settings. Well-founded self-reported measures save time and money in periods of restrained resources and enable a consumer-centred assessment when physical meetings are not possible.
The authors wish to thank all participants in the study. We also thank RG Active Rehabilitation and Veronika Lyckow for being valuable partners in this initiative. We acknowledge Professor Thórarinn Sveinsson (Department of Physical Therapy, School of Health Sciences, University of Iceland) for valuable statistical advice. Furthermore, we acknowledge professional translator Gunilla Lyckow, Noel Grehan and Tobias Lauritzen for assisting in the translation process.
Funding. This study was financed with grants from the Promobilia Foundation.
The authors have no conflicts of interest to declare.


 Click to show fullsize
Click to show fullsize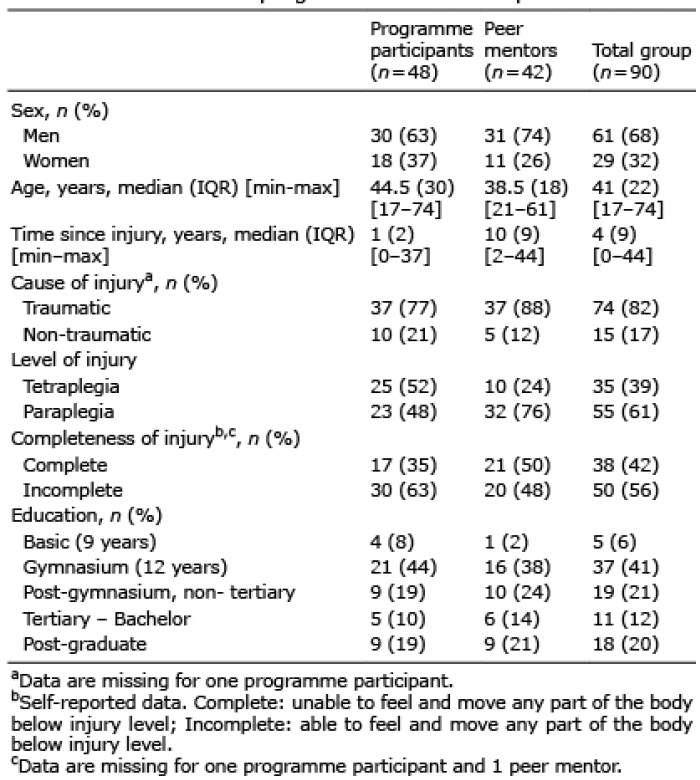 Click to show fullsize
Click to show fullsize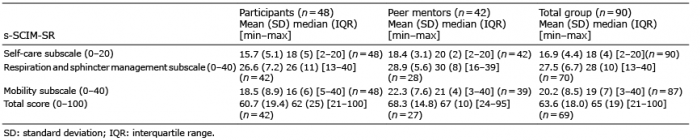 Click to show fullsize
Click to show fullsize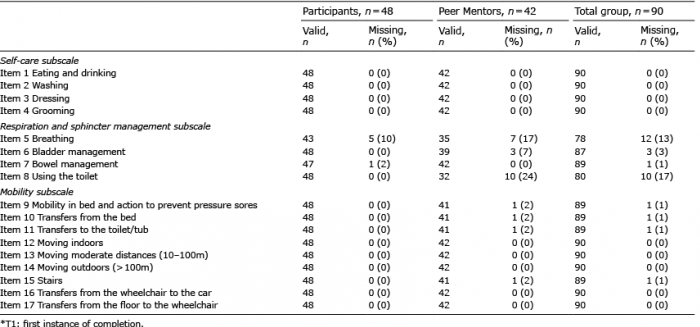 Click to show fullsize
Click to show fullsize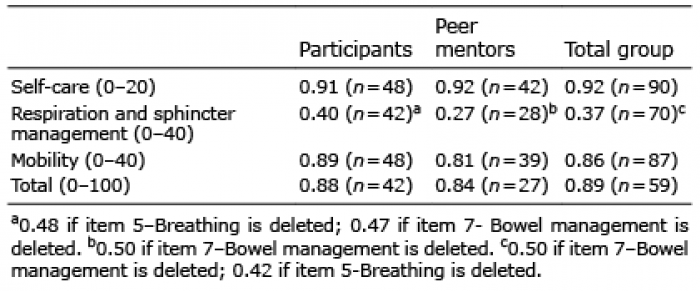 Click to show fullsize
Click to show fullsize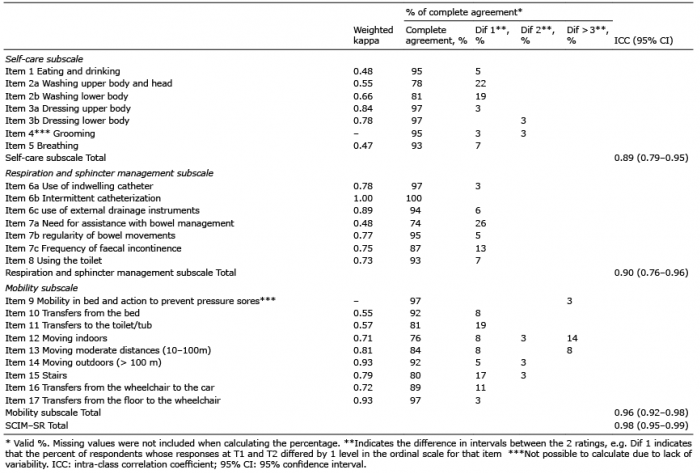 Click to show fullsize
Click to show fullsize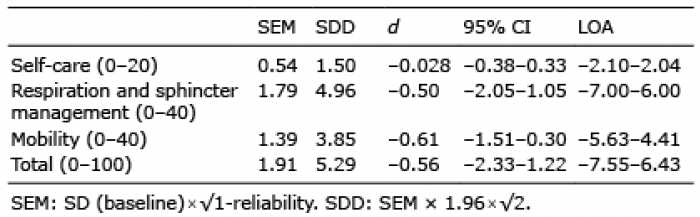 Click to show fullsize
Click to show fullsize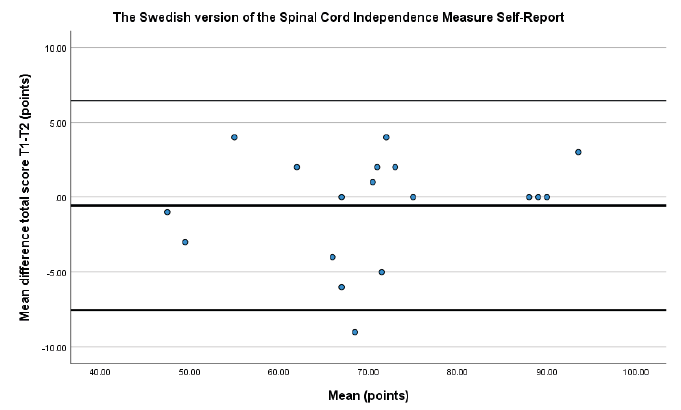 Click to show fullsize
Click to show fullsize